At the end of the 20th century, Portugal faced a major public health crisis as a surge in heroin use drove addiction rates, overdose deaths, and infectious diseases to record highs.
By the late 1990s, up to 100,000 people were estimated to be using drugs in a country of just 10 million, giving Portugal one of the highest rates of HIV in the European Union.
About half of new cases were linked to injection drug use, while rates of AIDS, tuberculosis, and hepatitis B and C were also on the rise.
As the issue devolved into a national crisis, officials noticed that criminalisation and marginalisation were fuelling the crisis rather than taming it.
In response, the Iberian country adopted the National Strategy for the Fight Against Drugs in 1999.
This new framework focused on a health-led approach, decriminalising personal drug possession in 2001 as well as expanding treatment, prevention, social reinsertion, and harm reduction services.
In the years following these reforms, drug deaths dropped sharply. Overdose deaths fell from 76 in 2001 to 10 in 2011 and have since remained among the lowest in the European Union. HIV diagnoses declined from 1,287 cases in 2001 to 16 in 2019, while the proportion of prisoners sentenced for drugs dropped from 40 to 15 per cent.
Hailed by many nations as one of the most effective treatment models in the world, Portugal’s strategy served as the blueprint for countries grappling with the same issue.
Among its early followers, officials across British Columbia began sketching their drug policies based on Portugal’s model, seeking to emulate its success.
Yet, 25 years later, a decade into a lingering public health emergency, with more than 18,000 drug deaths and a decriminalization pilot scrapped earlier this year, the province has failed to follow the European country’s footsteps.
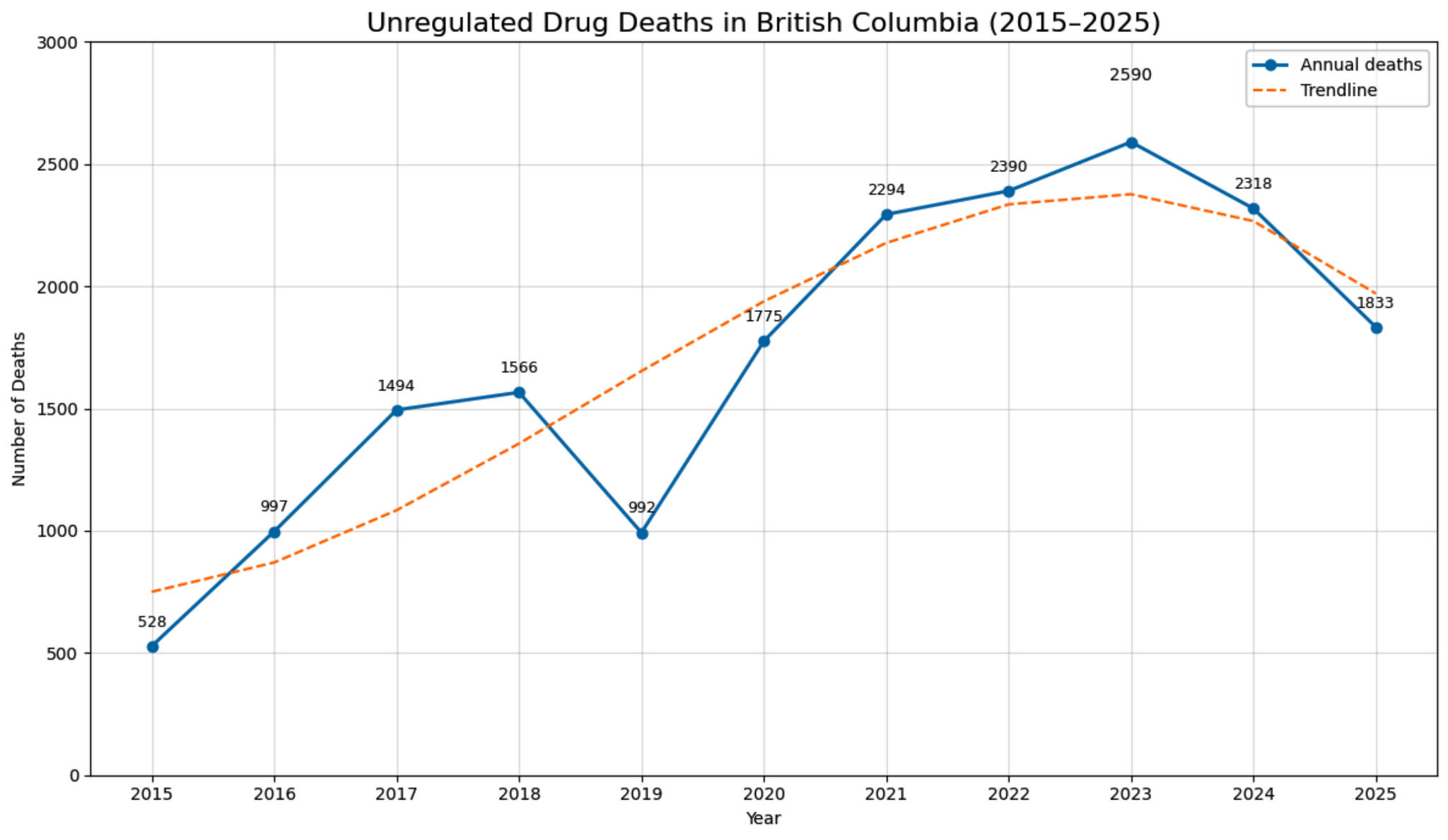
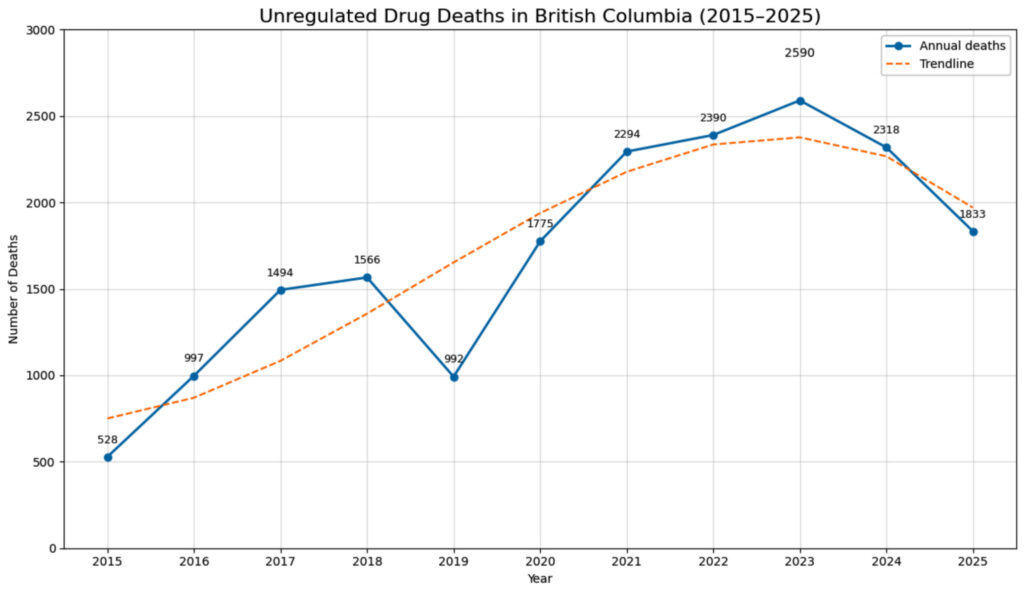
A graphic shows the number of unregulated drug deaths in B.C. from 2015 to 2025, spiking in 2023 with 2,590 deaths. (Data from BC Coroners Service)
Although B.C. aimed to follow Portugal’s lead, the effort ultimately failed, primarily because the two contexts are fundamentally different, explained researchers Karen Urbanoski and Bernie Pauly of the Canadian Institute for Substance Use Research.
Starting with the scope of the issue, the two are “not even comparable,” Urbanoski said.
In the early 2000s, Portugal didn’t contend with the same highly toxic and unpredictable drug supply as B.C.’s fentanyl- and benzodiazepine-dominated market, marked by increasingly lethal synthetic drugs.
With a drug market as deadly and volatile as B.C.’s, responding to the crisis requires substantially more resources, especially considering that, at their respective peaks, the province saw roughly 30 times more deaths than Portugal.
Beyond the toxicity of its drug supply, Portugal’s drug strategy paired decriminalization with a massive, coordinated investment in treatment, housing, and social support, whereas B.C.’s decriminalization came without enough detox beds, long-term treatment, supportive housing, mental health services or follow-up care, leaving major gaps in its response.
“Portugal had politicians and thought leaders who recognized the issue and that the response wasn’t just to decriminalize, but also to provide increased support,” said Pauly.
“It is very difficult to put policies into place if there isn’t any kind of political support.”
Additionally, Portugal’s model was implemented nationally and applied consistently, gaining both political and public support over time. In contrast, Canada’s system is fragmented vertically across municipal, provincial and federal jurisdictions, as well as horizontally through ministries, resulting in uneven enforcement of drug strategies, political pushback, and public opposition.
“It’s a complicated set of relationships and funding mechanisms which makes it genuinely more difficult to bring everyone onto the same page,” said Urbanoski.
“We need to have an effective coordinated treatment system and I would argue we don’t have one now.
“What we are currently doing is not effective.”
Beyond a fractured approach, both scholars noted a lack of willingness by the provincial government to implement policies they believe could help tackle the toxic drug crisis.
“Decriminalization is a good example of the government trying to implement an intervention that barely gets out of the very early stages,” said Urbanoski.
“The pilot hasn’t been resourced or scaled up to the point at which it could have a population health effect.
“It’s more of an implementation issue than an intervention effectiveness issue.”
Part of this reluctance may be explained by an unfavourable public perception, caused by a lack of proper education, unlike in Portugal, where awareness campaigns secured support from both politicians and citizens, said Pauly.
“Public knowledge really matters in terms of being able to scale up these interventions. Some research shows there wasn’t good public education around decriminalization in B.C.”
Warning against romanticizing Portugal’s drug strategy, which had “hiccups” in its implementation and a “fairly robust mandatory treatment component,” Urbanoski and Pauly reiterated that no country or context is the same.
While the path to success is unknown, the two scientists say B.C. can curb its toxic drug crisis. Their questions, however, remain when and how.
“How come we’re still in a public health emergency after a decade?,” said Pauly. “If you look around my office, you can see pictures of people I knew who have died. How many more are going to die?
“We have tools…but what are we willing to do? I don’t want to be sitting here 10 years from now and having this conversation again because it’s just not acceptable that we’re still in this place.”